Ozempic for menopause weight gain is one of the most searched phrases by women over 45 right now — and for good reason. You eat well. You exercise. You do everything right — and the scales barely move. If this sounds familiar, you are not failing. Your hormones might be working against you. Here is what science says about a new generation of medicines that are changing everything.
Ozempic for Menopause Weight Gain? Why Weight Loss Feels Impossible in Menopause
Before we talk about any medication, it helps to understand what is actually happening in your body — because it is not simply a matter of willpower or effort.
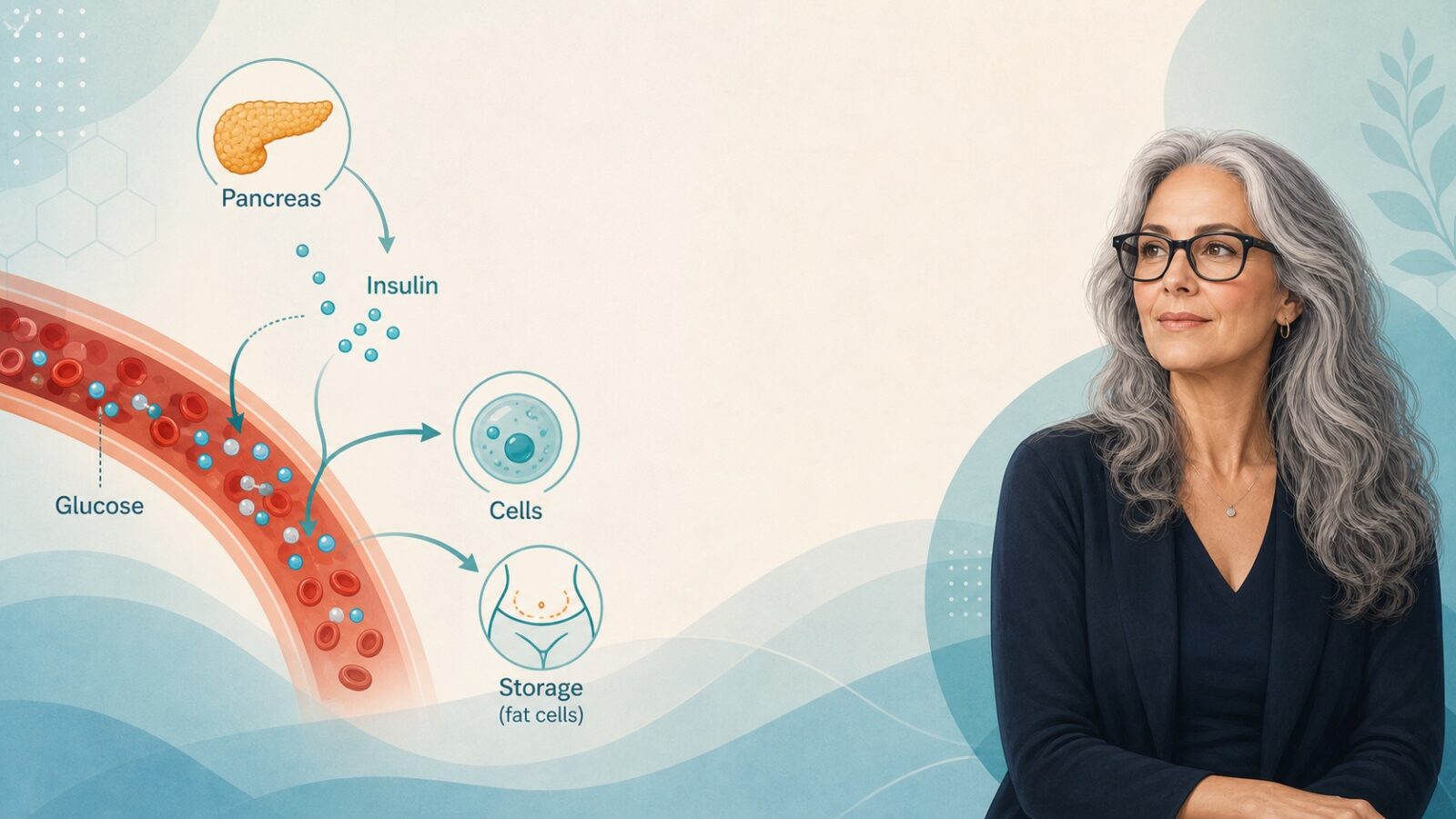
When oestrogen levels drop during perimenopause and menopause, something significant happens to the way your body processes sugar. Oestrogen — specifically a form called 17β-oestradiol — is a key regulator of how cells respond to insulin, the hormone that moves glucose out of the bloodstream and into your muscles and organs for energy. When oestrogen falls, cells become less responsive to insulin. This is known as insulin resistance.
In plain terms: your body produces insulin normally, but the signal is not being heard properly. Instead of glucose entering your cells to be burned as fuel, it stays in the bloodstream. The pancreas then produces even more insulin to compensate, which sends a powerful signal to your body to store fat — particularly around the abdomen. You can be eating a clean diet, swimming, walking, lifting weights, and still see barely any change on the scales. This is not a myth. It is biology.
Research confirms that insulin resistance is an independent predictor of weight gain in postmenopausal women — completely separate from how much you eat or how much you exercise. A major meta-analysis of 17 randomised controlled trials covering more than 29,000 participants, published in 2024, confirmed that declining oestrogen levels significantly increase the risk of insulin resistance in menopausal women — and that hormone therapy can actually reduce that risk. But for women who cannot or choose not to use HRT, or for whom HRT alone is not enough, a new class of medicines is now offering real, evidence-backed help.
What Are GLP-1 Medicines?
GLP-1 stands for glucagon-like peptide-1, a natural hormone your gut releases after eating. It tells your pancreas to produce insulin, signals your brain that you are full, and slows the rate at which your stomach empties. In people with insulin resistance, this system is not working as efficiently as it should.
GLP-1 medicines mimic or enhance the effect of this hormone. They are not appetite suppressants in the old-fashioned sense — they work at a hormonal level, resetting the way your body responds to food and manages blood sugar. The result, for many people, is that hunger decreases naturally, portion sizes reduce without feeling deprived, and — crucially — insulin sensitivity improves.
There are currently two approved options in the UK, and a third is in advanced clinical trials. Here is what you need to know about each.

The Three Medicines Explained
Ozempic (Semaglutide)
Ozempic is the brand name for semaglutide, a once-weekly injection developed originally for type 2 diabetes. It works by activating GLP-1 receptors, which increases insulin secretion when blood sugar is high, slows stomach emptying, reduces the liver’s release of glucose, and curbs appetite.
It is important to know that Ozempic itself is licensed for type 2 diabetes, not weight loss. The same drug at a higher dose is sold as Wegovy, which is the version licensed specifically for weight management. In clinical studies, Wegovy produced an average weight loss of around 13–15% of starting body weight.
Research published in a peer-reviewed journal found that semaglutide significantly improved insulin sensitivity, reduced insulin resistance, lowered fasting glucose, and promoted substantial weight loss. For women in menopause dealing with insulin resistance, this is directly relevant.
An important bonus finding: a study found that women using semaglutide in combination with HRT lost 16% of their body weight after 12 months, compared with 12% in women using semaglutide alone — a 30% relative difference. If you are already on HRT, the combination may work better than either treatment alone.
Mounjaro (Tirzepatide) — The More Powerful Option
Mounjaro is the brand name for tirzepatide, a newer weekly injection that works on two hormonal pathways simultaneously — GLP-1 and a second hormone called GIP (glucose-dependent insulinotropic polypeptide). This dual action is why tirzepatide typically produces stronger results than semaglutide alone.
Like Ozempic, Mounjaro was first developed for type 2 diabetes. In the UK, Mounjaro is now licensed for weight management directly. In clinical studies, tirzepatide produced average weight loss of around 20% of starting body weight — notably higher than semaglutide.
The data for women specifically is striking. A post-hoc analysis of the SURMOUNT clinical programme found that tirzepatide treatment was associated with significant reductions in body weight and waist circumference in women living with obesity. Data presented at the Annual Meeting of the European Association for the Study of Diabetes showed women lost an average of around 24% of their body weight on Mounjaro, while men lost around 18% — suggesting the medication may have particular benefits for women.
A January 2026 Mayo Clinic study found that postmenopausal women on hormone therapy who also took tirzepatide lost 35% more weight than women taking tirzepatide alone. This is still an observational study, so causation cannot be confirmed, but it is a compelling finding for women navigating menopause.
Retatrutide — The Next Generation (Coming Soon)
Retatrutide is a triple-acting experimental drug currently in Phase 3 clinical trials, developed by Eli Lilly. It targets three gut hormones simultaneously: GLP-1, GIP, and glucagon. This is why it is sometimes called a “triple-G” drug.
Phase 3 results from the TRIUMPH-1 trial — the largest and longest trial of this kind to date — showed that participants who stayed on the 12mg dose for 80 weeks lost an average of 28% of their body weight. Even the lowest 4mg dose produced 19% weight loss. For context, that is roughly double the results seen with first-generation GLP-1 drugs.
However, it is important to be realistic about timing. As of June 2026, retatrutide is not approved anywhere in the world. Eli Lilly is expected to submit to the US FDA in late 2026 or early 2027, with UK MHRA approval realistically expected in 2027–2028, and NHS availability potentially not until 2029 or later. It is something to watch, but not something you can access yet through normal channels.
Side-by-Side Comparison
| Ozempic / Wegovy | Mounjaro | Retatrutide | |
|---|---|---|---|
| Active ingredient | Semaglutide | Tirzepatide | Retatrutide |
| How it works | GLP-1 agonist (single pathway) | GLP-1 + GIP (dual pathway) | GLP-1 + GIP + glucagon (triple pathway) |
| Average weight loss | ~13–15% | ~20–24% | ~19–28% (trial data) |
| UK approval status | ✅ Approved (Wegovy for weight loss) | ✅ Approved (Mounjaro for weight loss) | ❌ Not yet approved |
| How taken | Weekly injection | Weekly injection | Weekly injection (in trials) |
| Main side effects | Nausea, vomiting, digestive issues | Nausea, vomiting, digestive issues | Similar — nausea, vomiting |
| Benefit with HRT | +30% more weight loss with HRT | +35% more weight loss with HRT | Data not yet available |
| Insulin resistance | Significantly improves | Dual action may improve more | Expected to improve (trial data pending) |
Ozempic for Menopause Weight Gain? What These Medicines Are Not
It is worth being clear about what these drugs do not do. They are not magic pills, they are not a replacement for a healthy lifestyle, and they are not right for everyone. Common side effects include nausea, vomiting, and digestive discomfort, particularly in the early weeks. They are prescription-only medicines, and the decision to use them should always be made with a qualified doctor who knows your full medical history.
They are also not cheap. Mounjaro and Wegovy are currently available privately in the UK; NHS access is being rolled out gradually through specialist weight management services. Costs vary but can run to several hundred pounds per month privately.
These medicines are also not a judgement on your choices. If you have insulin resistance worsened by menopause, your body is working against you in a very real biological sense. The research simply confirms what many women already knew: sometimes doing everything right is genuinely not enough, and there are now medical tools that can help.
The Menopause –Insulin Resistance Connection
To bring it all together: the drop in oestrogen that comes with perimenopause and menopause directly impairs the body’s ability to use insulin properly. This creates a cycle — higher insulin levels drive fat storage, particularly around the abdomen, which itself worsens insulin resistance further. GLP-1 medicines break that cycle by improving insulin sensitivity, reducing appetite at a hormonal level, and — when combined with HRT — may offer significantly greater results than either treatment alone.
If you suspect insulin resistance is contributing to your weight struggles, the first step is a conversation with your doctor. Ask about fasting glucose, fasting insulin, and an HbA1c test. These give a clear picture of how your body is handling blood sugar — and open the door to a real, evidence-based conversation about your options.
References
- Harvard Health: How does Ozempic work?
- Mayo Clinic: Tirzepatide and hormone therapy in postmenopausal women
- The Menopause Society: Hormone therapy and insulin resistance
- PubMed: The role of oestrogen in insulin resistance
- Scientific American: New GLP-1 drugs coming
- Second Nature: Retatrutide and the NHS
Disclaimer: This article is for information only and does not constitute medical advice. Always consult your GP or healthcare provider before starting any new medication.





